
今月のトピック
食事、栄養素、腸内微生物叢
20 9月 2017
これらは顕微鏡なしでは見ることができないが、私たち個人の微生物叢を構成する何十億もの微生物は、私たちの健康にとって非常に重要である。あなたが摂取する(または摂取しないことで)食物や栄養素がどのように微生物叢に影響するかを学ぶ。
11 7月 2017

トマトを調理することで、リコピンの吸収が高まることをご存知ですか?そして、サラダドレッシングの適度な脂肪が、サラダからのβカロテンや他の脂溶性カロテノイドの吸収を高めることをご存知ですか?
カロテノイドは、私たちが食べる野菜を始めとする多くの植物で自然に存在する脂溶性分子の一種です。これらは、このような食物の多くに黄色、赤色、橙色の色彩を与えます(1)。このような化合物は、さまざまなカロテノイドの種類によってそれぞれに異なる、健康上の利益が知られています。一部は、βカロテン、αカロテン、βクリプトキサンチンのように、プロビタミンA活性を持ち、体内でビタミンAに変換されます(2)。その他は、リコピン、ルテイン、ゼアキサンチンのように抗酸化活性で知られ、また目の網膜に存在しています(3、4)。どんな栄養素も、最適な健康上の利益を達成するには、どのような要素が、身体にどのように取り込まれるのかを理解することが重要です。
先進国では稀ですが、ビタミンA欠乏症は、依然として世界中で蔓延する深刻な問題です(5)。世界保健機関(WHO)は、2億5千万人以上の学齢期前の子供たちがビタミンA欠乏症に罹っていると推定しています。その結果、最大50万人の子供が毎年失明し、その内の半分は視力を失ったことより1年以内に死亡しています(6)。これらの多くの国々では、レチノールの形で既成ビタミンAを含む食物(乳製品、卵黄またはレバー)の入手が限られています。このため、ビタミンAの主要な源泉は、βカロテンなどのプロビタミンAカロテノイドです(7)。しかしながら、βカロテンから推定されるビタミンA活性の量に関しては、論議があります。その論拠として、主要な科学機関または規制機関は、この件に関して異なるガイドラインを公表しています(表1)。
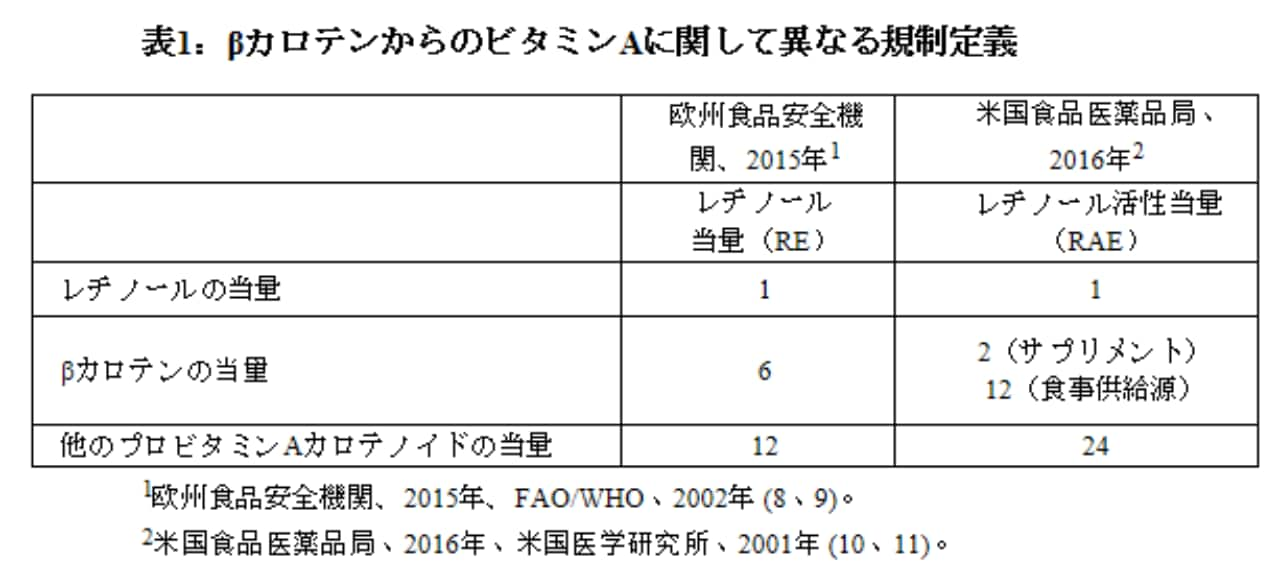
欧州食品安全機関の勧告は、国連食糧農業機関(FAO)/世界保健機関(WHO)の勧告に基づいた当量を使用していますが、一方、米国食品医薬品局(FDA)は米国医学研究所(IOM)の2001年のビタミンAの食事摂取基準に基づいた当量を使用しています。科学的合意とそれに続く規制声明が異なる理由は、カロテノイドのバイオアベイラビリティーに影響を与える可能性があるさまざまな要因により引き起こされた、科学文献から報告される値の変動に由来する可能性があります(12)。
予想されるように、異なるカロテノイドは、異なるバイオアベイラビリティーを示しています。これらは部分的には分子構造によるものですが、それぞれの吸収メカニズムにも左右されます(13)。一般的には、カロテノイドの用量が高いほど、吸収される割合は低くなります。油中の純粋なβカロテンを生理学的用量(約500μg)投与した研究では、約半分が吸収されたことが分かりました(14)。しかしながら、より多くの用量(約15mg)が試験された場合では、用量の約10~15%しか吸収されませんでした(15)。同様な傾向は他のカロテノイドでも観察されています(16)。
植物の成長時にカロテノイドが細胞に蓄積される方法も、カロテノイドのバイオアベイラビリティーに影響を与える可能性があります。カロテノイドの結晶構造、または植物細胞中の他の成分が腸管吸収のためのアクセスを抑制しているのかも知れません。このことは、植物の種の間でも異なる可能性があり、(17)、栄養強化された穀物も含まれます(18)。IOMの、純粋βカロテン(サプリメント)と食物中のβカロテンとの6:1の当量は、植物性食物マトリックス中のβカロテンを、食事と一緒にサプリメントとして消費される油中のβカロテン(19、20)、または焼きウェハース(21)、またサラダドレッシングなどの食物マトリックスに含まれるβカロテン(13、22)と比較した、いくつかの研究との関連により確立されました。しかしながら、これらの結果や、より最近に発表された研究が、かなり異なっていることを認識することが重要です。
予想とは反対に、調理された食品は実際にカロテノイドの吸収を高めます。高温ではいくらかの分解が発生する可能性がありますが、植物組織の加熱はバイオアベイラビリティーを大幅に向上します。これは植物細胞壁やその他のバリアを破壊し、カロテノイドの放出や吸収を促進することによる可能性が考えられています(23)。たとえば、生トマトと比較して、トマトペーストからのリコピン吸収の増加が見られます(24、25)。
食物や食事のその他の化学成分も、バイオアベイラビリティーに影響を与える可能性があります。食事性脂肪の存在はβカロテンの吸収を高めることが示されています。研究では、全脂肪サラダドレッシングを加えることは、低脂肪または無脂肪のドレッシングに比べて、カロテノイドの吸収を劇的に高めることが示されました(26)。また、アボカドなど他の食物由来の脂肪も、カロテノイドの吸収を高めることができます(27)。卵黄に見られるルテインは、バイオアベイラビリティーが高いことが示されており(28)、卵を生野菜と一緒に摂取することは、野菜からのカロテノイドの吸収を高めることに役立つことが示されています。
カロテノイドが摂取される食物の形態にかかわらず、個人間の生理的違いも、カロテノイドの吸収に影響を与える可能性があります。遺伝的要因が、カロテノイドのバイオアベイラビリティーにおいて役割を果たす可能性があるという認識が高まっています。βカロテン変換酵素BCMO1の違いが、各個人の反応にどのように影響を及ぼすかに関する展望は、3月の月間トピックを参照ください。BCMO1遺伝子の特定の遺伝的変異株を持つ各個人は、ビタミンA欠乏になりやすく、適切な量の既成ビタミンAの摂取を確実にすることが求められます(29)。体内の低ビタミンAの状況は、βカロテンのレチノールへの変換を増加させる場合があります(30)。体重は、血清カロテノイドのレベルに関連があり(31)、また肥満外科手術患者では、小腸の変化によるビタミンA欠乏が観察されています(32)。他のメカニズムが、キサントフィルに作用し始めるかも知れません。最近の研究は、ルテインやゼアキサンチンがLDLおよびHDLの粒子によって運ばれるため、リポ蛋白代謝における各個人の差が、網膜への送達に影響を与える可能性を示唆しています(33)。
それでは、これらの変数を前提として、どのようにすれば食事中のカロテノイドを最大限に活用することができるでしょう。もちろん、これまでに述べたすべての要因を管理することはできません。ただし、検討すべきいくつかの経験則があります。
色彩豊かな食事をとること:緑色、黄色、オレンジ、赤色の野菜や果物を習慣的に食べることは、カロテノイドの摂取を促進します。
調理すること:加熱は、カロテノイドの放出を最大化するのに役立ちます。
適度な脂肪を恐れないこと:油を使用する調理は、脂溶性カロテノイドおよび他の脂溶性ビタミンの野菜からの吸収を推進するすばらしい方法です。
食事のサプリメント:サプリメントを服用する場合は、食事と一緒に摂取してください。これはカロテノイドだけではなく、他の栄養素にも当てはまる良い助言です。
20 9月 2017
これらは顕微鏡なしでは見ることができないが、私たち個人の微生物叢を構成する何十億もの微生物は、私たちの健康にとって非常に重要である。あなたが摂取する(または摂取しないことで)食物や栄養素がどのように微生物叢に影響するかを学ぶ。
22 1月 2018
ビタミンCは、コラーゲン形成におけるその役割が最もよく知られており、ビタミンC欠乏症である壊血病の予防に不可欠です。最新の研究では、ビタミンCの摂取と体内レベルは、特定の慢性疾患のリスクに影響を及ぼす可能性があることが示唆されており、第一人者の専門家はより高用量を毎日摂取することを推奨しています。より詳細な内容を読む。
20 12月 2017
新しい年はニュースのヘッドラインを彩る複数のホットな研究エリアから始まります。2018 年の健康および栄養学の傾向についてご一読ください。